


Large Study Reveals Substantially Less Hospitalization, Death, ICU Admission, And Ventilation With OMICRON Compared To Delta


There’s a new study out from researchers at UC Berkeley, and Kaiser Permanante in California illuminating the current picture Omicron is painting before the public eye. That is, reduced symptomatic hospitalization, death, ICU admission, and mechanical ventilation compared to Delta. This publication will examine the particulars of that study, and the implications for personal risk reduction, public vaccine and masking mandates, school closures, and testing.
Looked to compare clinical outcomes of patients infected with Delta and Omicron
Endpoints measured were any hospital admission, hospital admission associated with new-onset acute respiratory symptoms, ICU admission, mechanical ventilation, and mortality
Study takes into account vaccination status, and previous infection
Study used SGTF RT-PCR as an indicator of Omicron (S- gene target failure is a hallmark of Omicron- essentially, it’s missing the S-gene and certain PCR tests show that)
Study used non-SGTF to identify Delta
Positive RT-PCR tests (n=69,279) were from Kaiser healthcare system
Total Omicron cases= 52,297
Total Delta cases= 16,982
DELTA (EVENTS PER THOUSAND): Any hospital admission relating to Delta= 222 (1.3%), symptomatic hospital admissions= 216, ICU admissions= 23, mechanical ventilation=11, death= 14 (see table. 1 below)
OMICRON (EVENTS PER THOUSAND): Any hospital admission relating to Omicron= 235 (0.5%), symptomatic hospital admissions= 182, ICU admissions= 7, mechanical ventilation= 0, death= 1 per thousand (see table. 1 below)
All of that means 53% reduced risk of any subsequent hospitalization, 53% reduced risk of symptomatic hospitalization, 74% reduced risk of ICU admission, and 91% reduced risk of death with Omicron compared to Delta
Median hospital stay in those with Omicron was 70% shorter compared to Delta totaling 3-4 days
Less Delta cases in those that were vaccinated
Vaccination status played little to no role in protecting against Omicron
Delta less detected in those with previous infection
Confounders: 1.) Follow up time for long duration hospitalization was limited- mean length of follow up for Omicron patients was 5.5 days. Mean length of follow up for Delta was 15.8 days. 2.) Incidental detection of Omicron in hospitalized patients is likely higher considering the time of testing as Omicron took over Delta in case numbers. 3.) Access to testing for Kaiser members differs VS. general population (possibly greater access to tests as a Kaiser member). 4.) Prevalence of vaccination and prior infection in Kaiser patients compared to the general populace may effect transportability of effect size estimates.
Finally, 2 nice visuals for you. The first in the form of a purple and green graph. The second, and a numbers chart. NO SGTF is Delta, SGTF is Omicron (see below)
From this study we see the variant in question is considerably less likely to hospitalize recipients, end peoples lives, land someone in the ICU, or require individuals to become ventilated. Alternatively, Omicron remains less lethal with a proclivity to spread regardless of vaccination status, natural immunity or current mitigation tactics. Considering all salient facts, a conversation needs to be had about 2 items. One, personal risk reduction. Two, public health policies for COVID-19.


What you can do to reduce your chances of severe disease from COVID-19:
First, obesity is the leading risk factor for severe COVID symptoms. It is time for those considered over weight to try and reduce that risk factor by making changes sooner than later. To explain, gym sessions, dieting, mountain climbing, power-walking, yoga, genetic testing with applied gene specific interventions, mental health therapy, and of course the treadmill are places to start. All together, those can help reduce obesity.
Just so you know, individuals that didn’t regularly exercise in a peer reviewed observational study, were at a 2.26 times increased risk of hospitalization, and 2.49 times increased risk of death from COVID-19 compared to those that exercised regularly. The parameters, brisk walking, and mild physical exertion with light weights for around 150 minutes per week. Just so we’re clear, thats FIVE 30 minute gym sessions, or TWO 60 minute sessions plus ONE 30 minute session.
While we’re on the topic of exercise, it is important to note one compelling lesson i’ve learned from my patients. That is, exercise was always easier for them with friends. Probably because there is accountability and companionship involved. Make it a team effort. Of course, diabetes, hypertension, and heart disease play a role in severe COVID outcomes. However, by applying the tools previously explained, you can also ameliorate signs and symptoms of those diseases as well. As a matter of fact, one could reduce most if not all risk factors by finding the right balance of diet, exercise, and mental health help.
Second, you could get vaccinated if you want. To set the table, healthy individuals with no co-morbidities or risk factors are afforded an infinitesimal likelihood of suffering severe disease or death from COVID-19. Now, even less with Omicron. With that said, vaccination should be a personal choice as one size fits all medical procedures are often deleterious and damaging in nature. That is because not all individuals are the same, therefore their bodies should be treated differently. Essentially, a 70 year old with many co-morbidities shouldn’t be advised on vaccination the same way a healthy 20-50 year old should be. As a result, vaccination for those who willingly receive will be granted reduced mortality and severity of disease. On the other hand, those young and healthy people who chose not to vaccinate already have supreme protection from the virus. So adhering to current broad vaccination guidance may not be appropriate for them.
Third, high risk individuals (immunocompromised, cancer patients, etc…) could consider the possibility of vaccination. The risk of being hurt by the virus in this cohort is much higher compared to possible side effects from a COVID vaccine. All and all, the immunity conferred by vaccination could be life saving. Again, personal choice.
Fourth, masking can reduce symptomatic seroprevalence by 11.2%, that evidence by a cluster-randomized trial out of Bangladesh. The previously mentioned is the only appropriate data in existence that justifies masking adults (not children). Interestingly, the study showed no net benefit to using cloth masks. If you feel inclined, masking is something that can help reduce the chances of contracting COVID-19.
Now that risk reduction has been examined, public health policy needs to be investigated. Let’s start with a tweet from the CDC Director Rochelle Walensky.

The implication from the CDC Director’s tweet is that Omicron is less severe in most ways, so it’s time to live with this. That said, living with this equates to changes in public health policies. Specifically regarding vaccine + mask mandates, school closures, and testing.
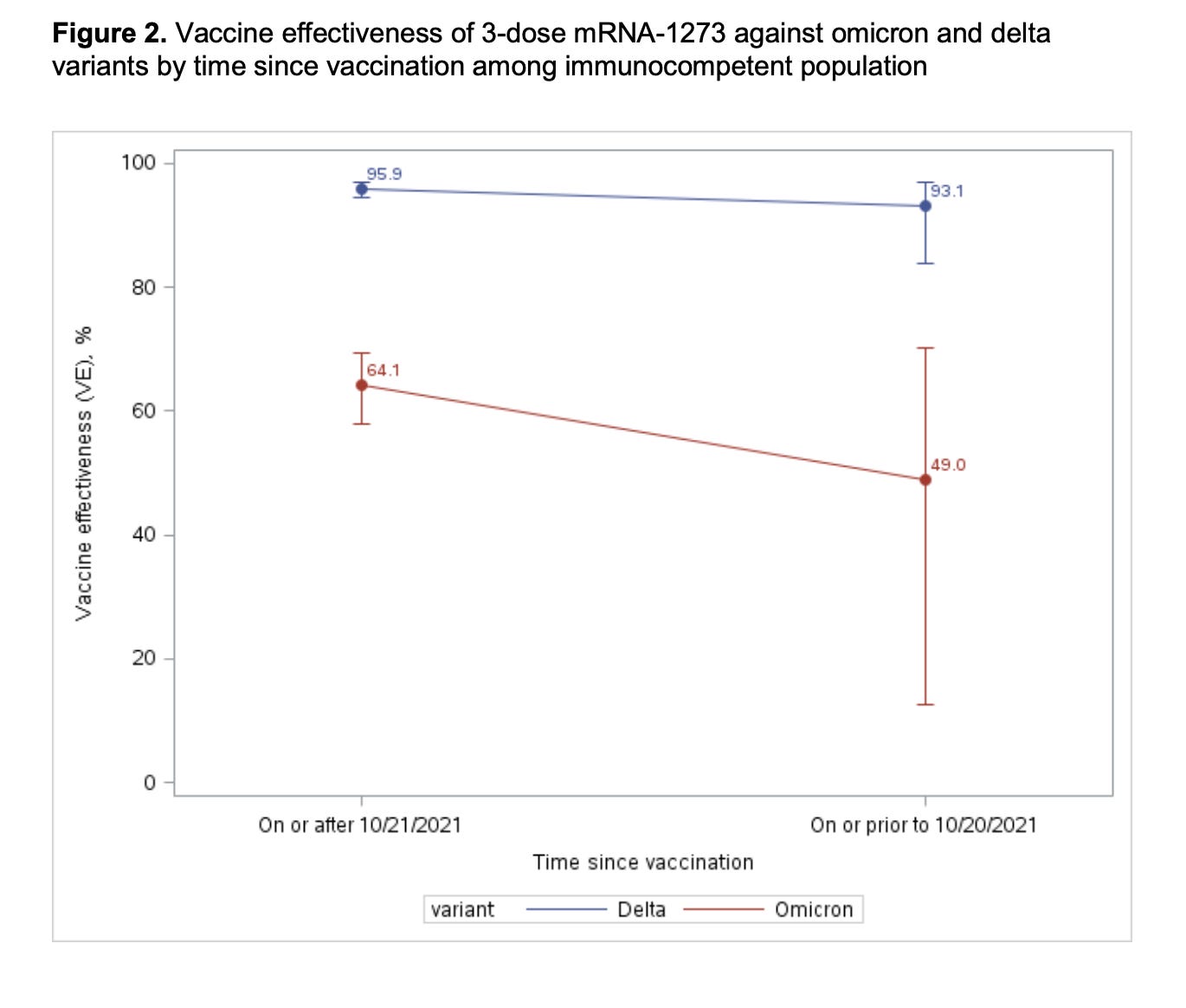
You see, as vaccines and boosters are substantially less effective at reducing the transmission of Omicron, Biden’s mandate is no longer justified. I wrote about this previously. To explain, coercing the public into getting a treatment that is not very effective against this circulating variant, which if anything, has shown to deliver a reduced risk of symptomatic hospitalization by 53%, ICU admission by 74%, and death by 91%, is inappropriate and goes against science. Speaking of the science, check out the graphs below. The effect of dose 1 and 2 plus boosters against Omicron are next to useless, see for yourself.

Moving on, many schools and daycares require masking of their enrollees. The problem, most encourage cloth masking which doesn’t work. Again, the only appropriate data to support masking is for adults in the Bangladesh study mentioned earlier. Importantly, the aforementioned cluster randomized trial demonstrated cloths masks were ineffective, and that surgical masks reduced symptomatic seroprevalence by around 10% in adults, NOT CHILDREN. Nonetheless, children in daycares continue to suffocate in cloth masks during their stay while simultaneously epidemiologists urge against using them. Interestingly, there’s a push for this same cohort to wear N95s, and KN95s now because of Omicron. Again, there is no data in existence showing efficacy for such an intervention. Oppositely, the data supporting supporting surgical masks, N95s, and KN95s pertain to adults, NOT YOUNG CHILDREN SPECIFICALLY. You should understand the largest benefit derived from using N95, and KN95s come from their ability to fit snugly on a face. Mark these words, it is impossible to properly fit a large N95 or KN95 on the face of a child. Additionally, there are no clinical trails to show the smaller sized ones reduce the spread of Omicron in kids.
About school closures. The reality is most children, teachers, and administrative staff are vaccinated and boosted, which protects them from severe disease. Regardless, the science now shows they will meet Omicron. Delaying the time until the virus is met serves no purpose anymore and is a detriment to public health. Early on during the pandemic when there were few treatments and tools available to combat COVID, school closures were justified. Interestingly, despite current closure, isolation, and vaccination status, Omicron continues to spread at an unprecedented rate. This all needs to stop.
Many say isolating staff and students helps the hospital surge. Sadly, closing academic institutions, and pivoting to online learning, forces nurses and doctors to remain at home and watch their kids which further exacerbates hospital shortages. Moreover, another study shows that closing schools has substantially diminished educational quality, and hastened neurocognitive decline in young children- they will not recover from this by the way. The cost of closure no longer justifies the risks.
Next, we can not test our way out of a pandemic. Again, the obsession with testing asymptomatic workers and asymptomatic healthy young students further worsens the educational and mental health crisis. Moreover, wasting tests on people with no symptoms eats up resources. Tests are already scarce because of this. It needs to be understood that the virus is becoming endemic, so obsessive BINAXING OR PCR-ING no longer yields a net-benefit like it used to, especially when vaccines no longer reduce mild symptomatic illness, and everyone has a date with the virus.
At this point, you’ve read everything and learned 3 things. Namely, how Omicron is affecting the population, ways to reduce your risk of contracting severe COVID-19, and public health policies that need to change in light of the new variant. Be that as it may, what do YOU feel should change?
LETS CONNECT: