


Masking School Children Isn’t An Intuitive Intervention Nor Is It Based In Science

In medicine, we don’t do things because they seem intuitive, we need evidence before we act. That said, every drug, therapy, and even medical device is subject to rigorous testing through a standard protocol otherwise known as a randomized controlled trial. RCTs help illuminate harms and benefits. Masking school children is not excluded from this process.
Just so we’re clear, and so the terms are understood, an RCT measures the effectiveness of an intervention on a treatment group, against a placebo or control arm. Moreover, each participant is randomly assigned to a group which reduces bias in the trial, hence the term randomized. Next, the intervention, drug, or device, is tested on the treatment cohort. Soon after, the results are analyzed, then summarized. Finally, the data will be reviewed by peers (aka peer review), and if everything is kosher, that study will end up in medical journals like JAMA, NEJM, PUBMED, Nature Medicine, etc which will then be utilized by practitioners like nurses and doctors throughout clinical landscapes.
Now the important question. Was that the process masking children went through to gain approval? No. Unfortunately, justification of such an intervention was speculative in lieu of appropriate cluster randomized controlled trails. Just so you know, the only cluster randomized mask trail in existence was out of Bangladesh and showed an 11.2% reduction in symptomatic seroprevalence against COVID in adults from wearing surgical masks. That said, the only masking data we have is applicable to adults, not children. As you can see, the evidence for masking school children is non-existent, yet public health authorities try to justify it.
This is their first claim. They say masking is like a “medical parachute”. Specifically speaking, not using a parachute while sky diving will surely increase the risk of death by nearly 100%. Therefore, no randomized controlled trial is needed to justify their use. The benefits are so much greater than the harms, it’s just obvious. Now, envision masking school children through the “medical parachute” lens. Why bother with an RCT when it’s obvious the barrier from masking can reduce transmission which could greatly reduce the overall risk of harm from COVID-19? This is a very flawed, and dangerous way to approach science.
You see, there is only 1 causal pathway to harm in the parachute analogy- not wearing it. That can be accounted for by strapping on the device before hopping out of the plane. As you now understand, by addressing the singular causative factor, nearly all risk would be averted and likely no harm would result. Conversely, most diseases like COVID-19 have multifactorial etiologies or causal pathways to harm, so addressing only one is unlikely to substantially reduce the risk of harm by any notable difference. As evidence of that, after analyzing nearly 80,000 medical practices, only one demonstrated at best an absolute risk reduction of around 33%. In other words, a masking intervention alone is unlikely to reduce the risk of harm or death from COVID-19 by any substantial order of magnitude because there are so many variables contributing to the transmission, and pathology of said disease. The child in the video below doesn’t believe that the benefits from masking outweighed the harms at school even though our public health officials want you to believe different. “It literally ruined our lives”, she cried (tap below to watch).

Next, in light of omicron, there has been a recent push for school children to wear N95s. Authorities claim they are better at protecting against the new and highly transmissible variant. Yet again, there is no evidence to support such a claim. Importantly, there are no officially rated N95 masks for children, they’ve only been validated for adults.
You should know this though. In general, for an N95 to be effective, an individual would have to secure the mask to their face without touching it after, then completely resist reorienting it. That’s because the key to an N95’s high filtration rate is its ability to create a vacuum-like seal between the mask and face at all times within high exposure environments. However, they will not work as well if tampered with. That said, there are 2 reasons N95s will not work for children in school.
One, kids will need to remove masks to eat and drink in school, use the water bubbler, etc (there are many more scenarios). For that reason, the suction will be broken leaving the child exposed to the virus.
Two, effective N95s fit properly. Unfortunately, these masks are much too big for a child’s face, so wearing them in school would only increase exposure to the virus. First the awkward fit would encourage the child to reorient the mask constantly, thus moving the viral particulate from the mask to their hands, their pens, their backpacks, their cell phones, you get the idea. Second, improper fitting masks have gaps which would allow the free flow of unfiltered air in through the mouth and nasal passages. It is important to note, “child sized” N95s have not been validated by any government authority, and have not been subject to randomized controlled trials.

Ultimately, because of the fitting issues, N95s will not afford children better protection at school. Instead, they hasten the contamination process and increase the chances of a child tracking the virus back home. All and all, considering that the single largest vector of transmission is the household, and that children being children will contaminate everything they get their hands on in the house, the virus will reach everyone in the domicile. Later that day/week company will be invited over to the now contaminated household; a family member, a friend, a repairman, Doordash.... Unfortunately, the virus will spread to them, then they will spread it to others, so on and so forth. As you can see, masking school children isn’t as intuitive as most may believe.
Moving on, N95s are approved for one use. In hospital settings when dealing with certain pathogens, we use them once then throw them away. I would never treat my tuberculosis patient, leave the room, then meet another patient with the same contaminated mask. Not only is that unsanitary, it is unethical and such malice would warrant the loss of my license to practice. Be that as it may, most children will end up reusing the same N95 due to lack of access or funds and therefore will perpetuate the same disease we seek to eradicate. Tuberculosis or COVID-19 alike, you don’t re-use masks.
Next, omicron is highly transmissible and regardless of vaccination status is spreading like wildfire. That is because there are approximately 51 total mutations, 30 of which are on the spike protein, and 15 on the receptor binding domain. To put things in perspective, delta was highly transmissible from 7 mutations. Omicron presents with a half hundred. Luckily, symptoms are usually mild from this variant, and school children handle it best statistically. After all, compared to delta, theres a 53% reduced risk of symptomatic hospitalization, 74% reduced risk of ICU admission, 91% reduced risk of mortality, and an infinitesimal chance of being ventilated with omicron. For those reasons, it no longer makes sense to delay meeting the virus by masking school children, especially with N95s. Everyone has a date with omicron.

Importantly, if masking school children was so intuitive there wouldn’t be so much conflicting guidance. To explain, the CDC recommends masking all children 2 and up, while the WHO and UNICEF advise against masking children 5 and under. Furthermore, for those 11 and under in certain circumstances, masking is encouraged. To revert back to the Bangladesh cluster randomized trial yet again, cloths masks did nothing to reduce the spread of SARS-CoV-2. The authors indirectly noted they were little more than decorations. Ironically, nearly 2 years later after advocating for them, CNN came out and admitted cloth masks were useless in curtailing the spread of the virus. Tap below to watch.

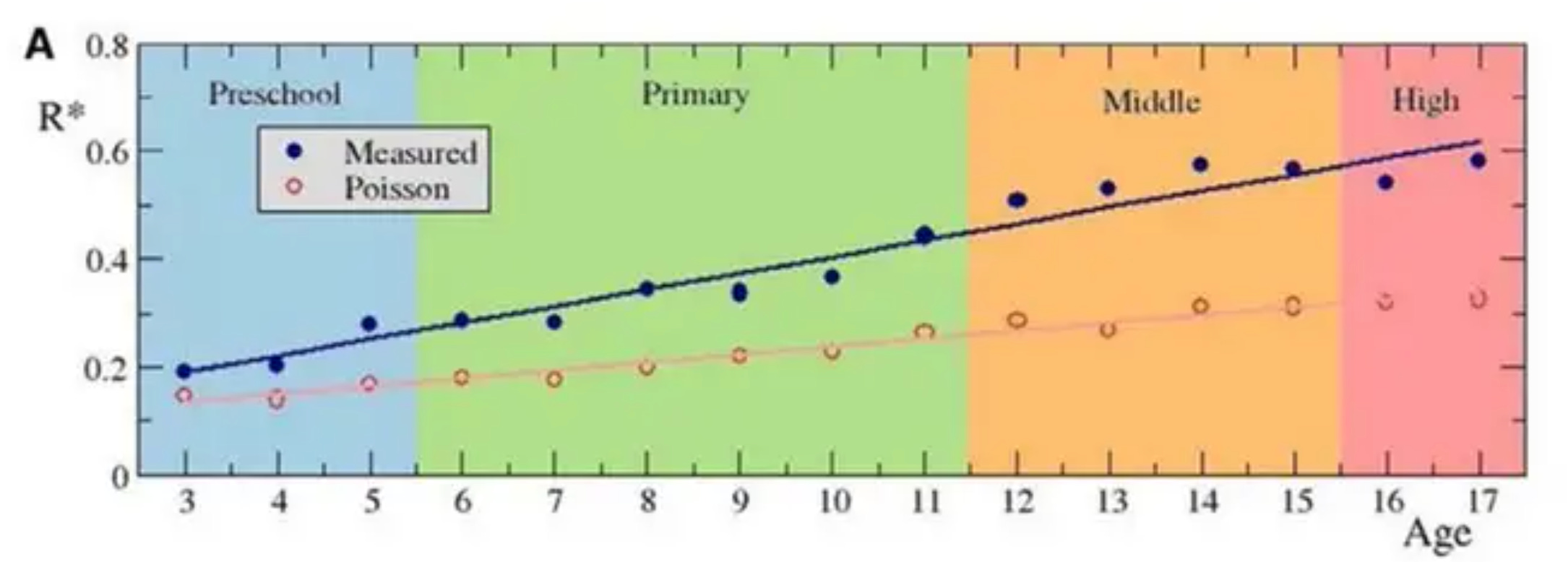
The United States seems to be ignoring a very relevant masking study from Spain. Notably, the image below shows the R value by age. Essentially, the R value is a way to rate the ability of the virus to spread. So, if the value is high, cases will keep increasing. Opposite to that, a reduced R value correlates with lesser cases. Kid in this study were masked age 6 and up. Knowing that, if masking worked, you’d see a decrease in the R value. Unfortunately that is not the case, the line keeps increasing. The point is, masks don’t work well for kids.
Let’s look at some harms caused by masking school children. There is now data to correlate neurocognitive decline in kids from COVID-19 measures like masking, school closures, and Zoom schooling. As you can see, in 2020 when the pandemic began, verbal and non-verbal development quotients dropped. Regrettably, this is irreparable damage most will never fully recover from. In a previous publication I explain how the ability of someone to use words, express concepts, and reason can be measured by verbal development quotients. Also, the ability of someone to critically think and problem solve using only visual data received from the environment can be measured by non-verbal development quotients.

Considering all of this, masking school children clearly isn’t an intuitive intervention. However, it is harmful, confusing, and non-scientific. So for that reason public health officials and schools need to eliminate masking requirements for young children.
LETS CONNECT: