


New Shocking Study Associates Increased Cardiac Arrest Events With Both Vaccine & COVID-19 | Evushield Monoclonal Antibody Reduced The Risk Of Covid Death By 50% | New Severe Covid Mechanism Found

You won’t hear the headlines listed above on the news, yet they happen to be of substantial consequence. That said, the data within this publication and summarized below gives important insight into the deleterious effects of both Covid-19 and mRNA vaccines
To explain, a new study released within the past ~24 hours explained how increased cardiac arrest events occurred during the pandemic and concurrently during a time of increased vaccine consumption & COVID cases, compared to before the pandemic. Next, new randomized control trial data from a recent Evushield monoclonal antibody trial denoted how the risk of COVID death was reduced by 50% when treatment was given early to recipients with mild to moderate illness. Finally, new science revealed another probable mechanism causing severe COVID
All and all, the data has been summarized below for you. Nonetheless, please read ALL references attached. As a last word, please share this vital information with friends and family so the truth gets out
A single-center retrospective study examining all out-of-hospital cardiac arrest (OHCA) patients before & during COVID (8/2019-6/2021) transferred to Lincoln Memorial Hospital, NY, revealed a nearly 31% increase in OHCA witnessed cardiac events during the pandemic VS before
All and all, this and other similar data suggests a notable increase of cardiac events during the COVID pandemic VS before (86% VS 55%, p = 0.03) implying the possibility of both vaccine and virus involvement
https://www.medrxiv.org/con.../10.1101/2022.06.08.22276169v1

A phase 3, double-blind, randomized, placebo controlled trial named TACKLE including 910 people, demonstrated that Evushield (tixagevimab & cilgavimab), a combination 600 mg IM monoclonal antibody injection, reduced the risk of severe COVID & death by 50.5% (RRR) with an ARR of 4.5% (95% CI 1·1–8·0,p<0·0001)
https://www.thelancet.com/.../PIIS2213-2600(22.../fulltext

New insight into a mechanism triggering the hyper-inflammatory pathway driving severe Covid shows how α2,6-sialylation was up-regulated in plasma samples along with an increase in associated excess compliment deposition in affected tissues from biopsies (lungs, heart, liver, kidneys)
https://www.medrxiv.org/con.../10.1101/2022.06.06.22275981v1

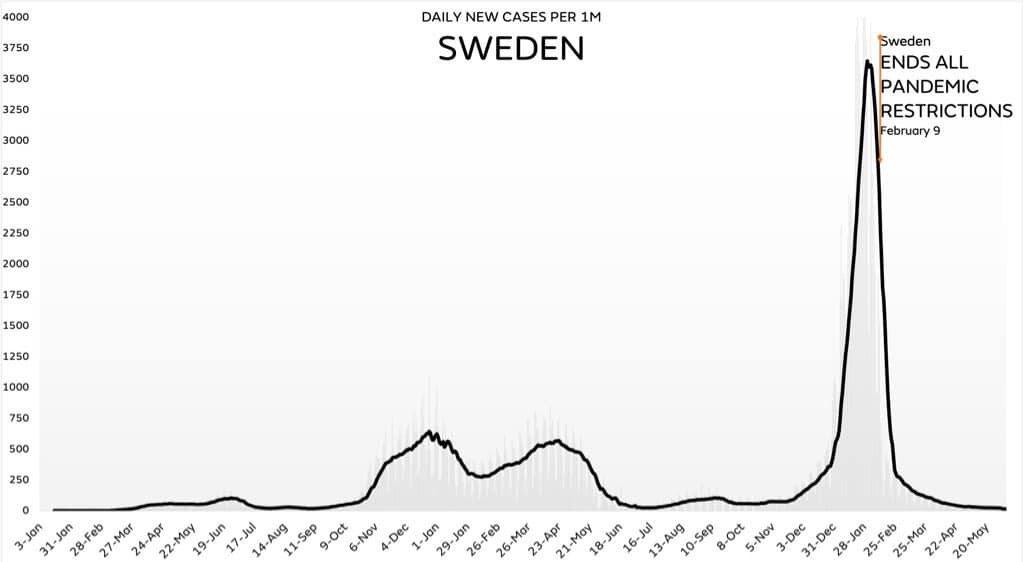
4 months ago Sweden ended the remainder of their pandemic restrictions and since then have been on record as having some of the lowest COVID case rates worldwide
LETS CONNECT:
Dr Carrie Madej has expressed huge concerns about monoclonal antibodies- 1) in how they are created and 2) longterm outcomes...
Many people don’t take into consideration how MA are created-
IMHO, we all need to be better informed on what we allow into our bodies whether it is a “vaccine”, monoclonal antibodies, painkillers, or medication.
All at risk people should have received a dose of monoclonal antibodies. But, as a physician I was not “allowed” to do this for several reasons. Peer judgement (lack of education and understanding) and fda/big pharma controls on prescribing monoclonals. We had monoclonals sitting in the pharmacy, not being used. But could not use it on a single patient in the hospital…. Because it’s not approved for in hospital use. I can’t think of a group of patients more at risk than those IN the hospital. (Mostly hospitalized with illness other than covid).