


New Study Found A 9-Times Increased Rate Of Myocarditis In Males After mRNA Booster | 3 Or More COVID-19 Vaccine Doses Associated With A 6-Fold Increased Risk Of Infection Said Cleveland Clinic | ETC

Very important data appeared over the past days that was suppressed by the media. Specifically, two new shocking studies were released that associated mRNA COVID-19 vaccination with higher than previously estimated rates of myocarditis, and higher than previously reported risk of infection.
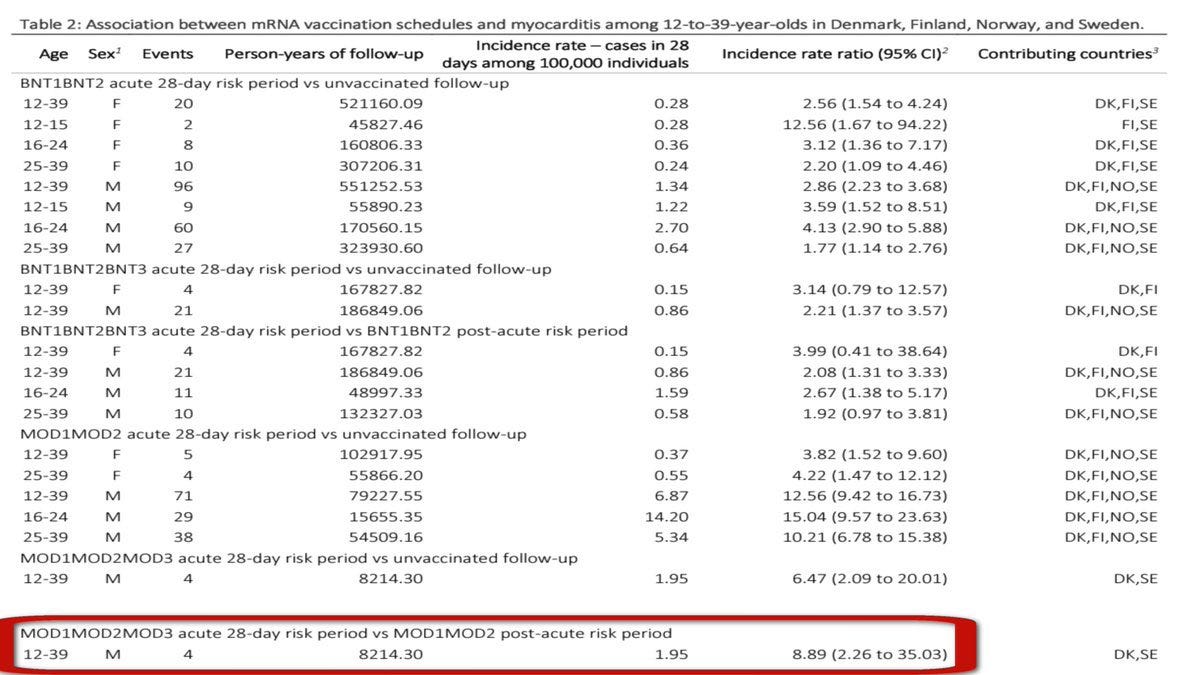
Start here. A new Nordic study found males aged 12-39 who took a Moderna COVID-19 booster compared to a second dose experienced a 9-fold increase in the risk of myocarditis. It should be noted, the previously mentioned figure was based on populations from Denmark, Finland, Norway, and Sweden who have recently stopped recommending mRNA vaccines for males under 30.
Next, a very prestigious medical institution named The Cleveland Clinic published new data that revealed every COVID-19 vaccine dose increased the risk of infection 6X- much higher than previously documented. The results are harrowing.
There is much more covered in this publication.
Of course, all data are summarized for you below. However, please read the sources. Finally, please make sure you share this bombshell new data by clicking the button immediately below so the truth gets out!
New Study Found A 9-Times Increased Rate Of Myocarditis After mRNA Booster
A new Nordic study of 8.9 million found a nearly 9-times increased rate of myocarditis 28 days following a 3rd dose of Moderna's mRNA booster VS dose 2 (8.89, 95% CI: 2.26-35.03) in males 12-39 from Denmark, Finland, Noway, and Sweden. Beware of boosters.
It should also be noted, for quite some time the medical literature illuminated a high risk of myocarditis for young males after dose 2 relative to dose 1. However, this study brought to light the importance of increased risk associated with dose 3 VS 2.
https://www.medrxiv.org/content/10.1101/2022.12.16.22283603v1
3 Or More COVID-19 Vaccine Doses Associated With A 6-Fold Increased Risk Of Infection Said Cleveland Clinic
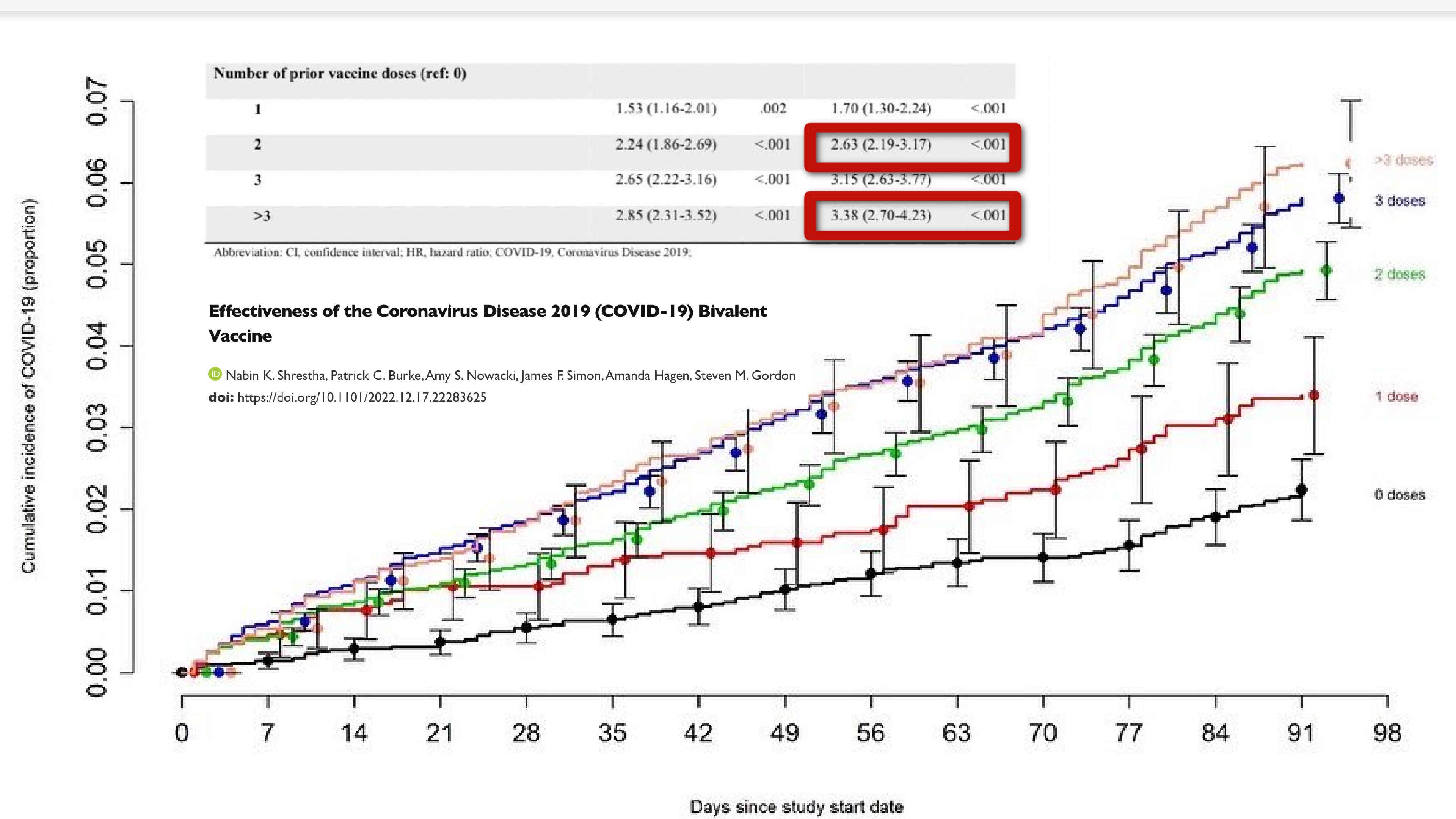
A new study from Cleveland Clinic of 51k healthcare workers found the more vaccine doses, the more incidence of covid infection. Those who received three or more doses had a 6-times increased risk of infection VS being unvaccinated.
Another important point from the study, bivalent vaccine effectiveness against infection was only 30% after only a few months.
Next, after 2 doses there was a 2.6-fold increased risk of covid-19 infection, and 3.38-fold increased risk after 3 or more doses.
https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1
Biden’s Federal Vaccine Mandate For Contract Workers Shot Down
Today freedom won. The 5th Circuit Court of Appeals shot down Biden’s COVID-19 vaccine mandate for federal contractors. "Today is a victory for freedom. We will continue to stand up against these abuses of power that threaten us now and in the future.”
agjefflandry.com/Article/13102

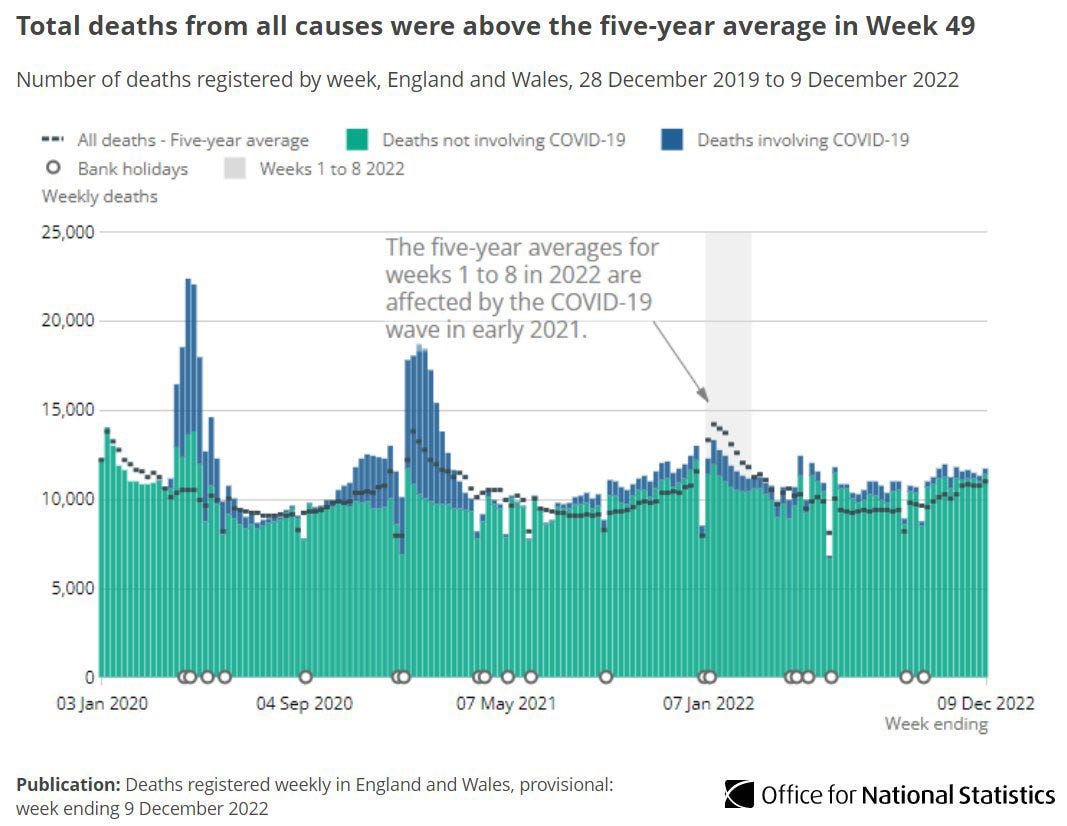
Reported Excess Deaths In England & Wales Up 6.2%
By December 9th 2022 there were 11,694 deaths, and 687 excess deaths registered in England and Wales which was 6.2% above the five-year average. This trend has continued for nearly 4 months.
LETS CONNECT:
Please pay attention - in the study below (Investigation into the toxic effects of graphene nanopores on lung cancer cells and biological tissues):
Heart tissue showed chemodectoma, toxic myocarditis, reddish brown atrophy; yellowish brown pigments suggesting lipofuscin granules as remnants of cell organelles and cytoplasmic material.
https://www.sciencedirect.com/science/article/pii/S2352940718302853 Investigation into the toxic effects of graphene nanopores on lung cancer cells and biological tissues
However, inhalation of graphene structures is believed to be a risk factor for cardiorespiratory disease. For example, inhaled graphene nanoplatelets can be transported deep within the distal regions of the lungs and trigger chronic inflammation in the respiratory tract. It is generally thought that the placenta, lung, gastrointestinal tract and skin act as major barriers for many nanostructures entry into living organisms. Indeed, a recent study on mice demonstrated that intratracheally delivered few-layered graphene was mainly retained in the lung, with 47% remaining after 4 weeks and this resulted dose-dependent acute lung injury and pulmonary oedema. An in vitro study of the effects of graphene and graphene oxide on human skin HaCaT keratinocytes demonstrated that oxidized graphene was the most cytotoxic, inducing mitochondrial and plasma-membrane damage, and suggesting low cytotoxic effects at the skin level. Reduced graphene oxide is more toxic than graphene oxide as evidenced by many studies reported recently. This is primarily due to its sharp edges and structural morphology. In contrast to the typically soluble nanoparticles examined in conventional toxicology investigations, graphene nanostructures have different shapes and surface areas, and which in turn can significantly influence their diffusion, dispersion, aggregation and agglomeration in plasma. Importantly, these “tunable” characteristics of graphene account for the varying toxic outcomes on the tissues. In vivo, following toxicity testing of graphene, post-mortem histological examinations of liver alterations have revealed hypertrophy of hepatocytes, necrosis and inflammatory cell infiltration in liver and kidney tissues.
Antioxidants act as a defense system to reinstate the cellular redox balance when oxidative stress is generated as a result of excess production of reactive oxygen species.
Disruption of this critical balance in the presence of excessive reactive oxygen species triggers the activation and promotion of a pro-inflammatory cascade, which in turn may cause mitochondrial release of proapoptotic factors potentially leading to cell death. Hepatocytes are key targets for reactive oxygen species damage, and therefore liver function and biomarkers of oxidative stresses should be investigated with great care.
Specifically, vacuolation, dilation of central vein and hemorrhage, vacuolation and dilation of central vein, damage of vacuolation, hemorrhage and degeneration of central vein, dilation of epithelial lining and hydropic degeneration oedema were observed in liver tissue. Kidney tissue of the treated groups showed acute vacuolization, dilation of epithelial lining, vacuolation and nucleus degeneration, nucleus damage, necrosis and epithelial degeneration.
Heart tissue showed chemodectoma, toxic myocarditis, reddish brown atrophy; yellowish brown pigments suggesting lipofuscin granules as remnants of cell organelles and cytoplasmic material.
The brain showed effects of secondary carcinoma, olegodendrocytoma small thin walled blood vessel and crytococcosis. Testicular tissue of treated groups showed spermatogenesis and vacuolation, dilation of germinal layer, degeneration of secondary spermatocytes, damage to the germinal layer and vacuolation. The lung showed damage of vacuolation, degeneration of central vein, inflammation, haemorrhage, d-shaped cells structure, hemosidophroages and lesion.
Indeed, 3D porous graphene frameworks have shown various effects from acute lethally to sub lethal toxic effects including histological, and oxidative stress responses and, after inhalation exposure in rats, graphene has been found to accumulate in the lung, leading to phagocytosis.
In this study, the first sign of toxicity recorded for the rats given an intraperitoneal injection of GNPs was an observed decrease in body weight at the higher dose. Toxic effects of GNPs on CBC were not observed although there was a slight (6%) reduction in platelet numbers in the 15 mg/kg group. The increased activities of AST, ALT, AMP and creatinine observed after 27 days are indicators of liver and kidney toxicity respectively and appeared in the rats receiving both single and multiple doses of GNPs, compared to control groups. Severe organ damage can increase the activities of ALT and AST and enhanced activity of both are observed when disease processes affect liver cell integrity. Importantly, increased serum ALT activity reflects specific hepatocellular injury. Histopathological alterations were also evident in the liver, where GNPs induced dose- and time-dependent histological alterations of the liver tissues, including congestion, prominent vasodilatation, and vacuolization.
The Nordic study also appears to show a 15x increase for myocarditis in the 2 dose Moderna males 16-24 relative to the unvaxed. Am I reading that correctly? And does that mean that the 8x increase (which uses a slightly different age grouping) is a multiplier of the 15x increase?