

Prior COVID-19 Infections Likely Account For More Immunity Than Vaccination - Pfizer & Moderna Need To Take A Back Seat
Prior COVID-19 Infections Likely Account For More Immunity Than Vaccination - Pfizer & Moderna Need To Take A Back Seat
Considering the data, immediate change is a necessity

The probability of someone receiving SARS-CoV-2 induced immunity from one of the many variants is substantially higher than protection gained from a limited amount of vaccine they’re allowed to receive. Meaning, most immunity against severe disease and death at this point has been conferred by natural infection, not current mRNA inoculation. That said, the jab needs to take a backseat while other interventions are focused on. Sadly, considering the facts stated above, proponents still continue to support the shots over more viable solutions.
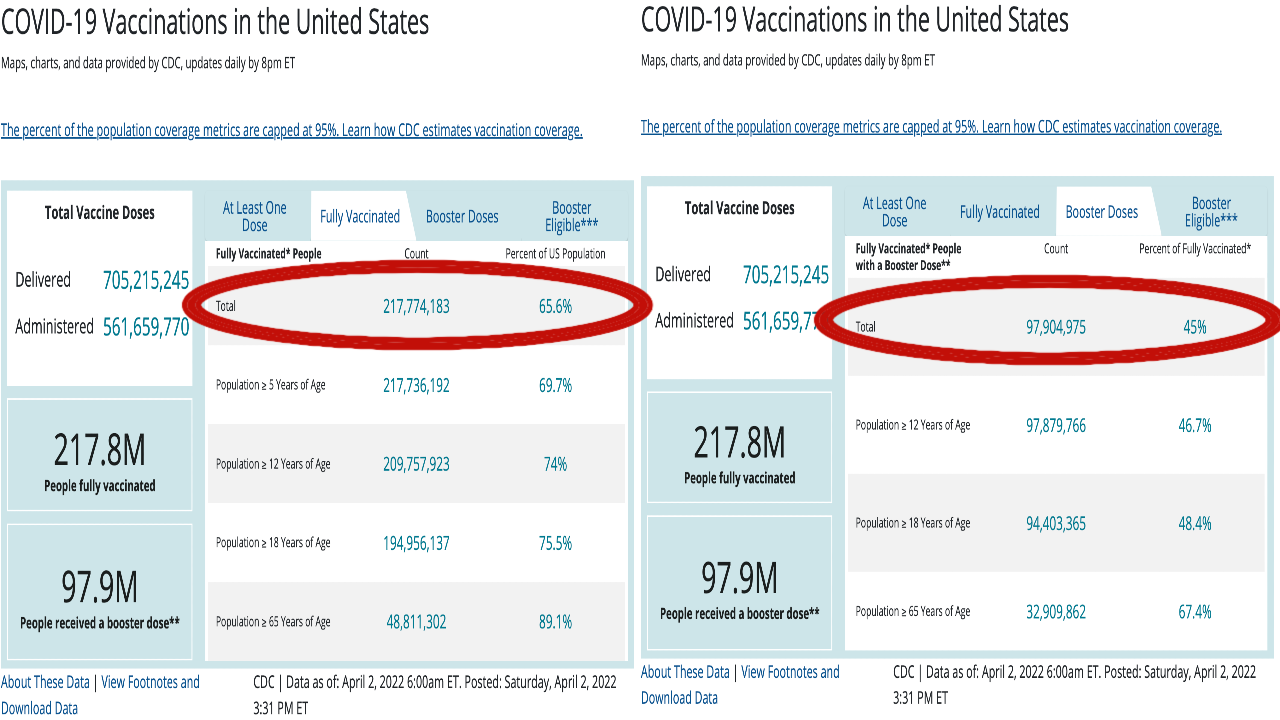
To begin, advocates of vaccination verbalize this first retort to the previously made statement. Specifically, there are 4 doses available and there were 4 COVID waves of substantial consequence, therefore the aforementioned proclamation is null. The simple response to this is that a 4th dose is not available for everyone. For instance, only those 50+ and individuals at high risk are afforded a 4th dose, while many children remain unable to receive any vaccine. Moreover, only 65% of Americans have received their primary series, while less than half have received a booster. Considering the facts, and that COVID infection does not age restrict, it is clear more people have access to infection than vaccination and therefore have likely been immunized by the virus more so than Pfizer & Moderna’s offerings.
Next, mRNA proponents state there isn’t enough seroprevalence/testing data to support such a claim regarding immunity. Sadly, they are mistaken. First, recent UK data revealed that in England 85.4% of 16+ year olds would test positive for COVID antibodies. Second, a recent CDC study illuminated that most children have been infected with the virus, a large number of which, because of age, are not allowed the vaccine. As you now understand, immunity in the form of antibodies, and CD8 + CD4 t-cells for many kids could only have been generated by direct exposure because a COVID vaccine had not been approved until recently. So, most protection was clearly gained via infection for nearly all children, not by vaccination.
“That’s incorrect!”, proponents would exclaim. Of course said advocates are wrong and blinded by bias. However, just so there’s no confusion, and so a final argument can be made, here are some facts to set the table:
Current COVID vaccines are engineered against the original Wuhan variant which is one of the main reasons efficacy against severe disease and death is not conferred from boosters. Luckily, and again, people have already received protection against severe disease and death from their first infection, or round of Pfizer or Moderna. Boosters are useless
COVID vaccines come with a higher risk profile of adverse events compared to others
In order to justify blanket suggesting a vaccine for the public, it needs to be more effective than simply preventing mild illness for a short period of time. Sadly, current COVID vaccines are not able to do this and regrettably present the risk of many side effects with less benefit than when first rolled out
There are no appropriate data that exist demonstrating a 4th dose reduction in severe disease or death because there are no randomized controlled trials in existence to show the aforementioned effect. Want to know why? Because Pfizer and Moderna didn’t run a randomized controlled trial for dose 4. Instead, inferior observational data from Israel with shady secondary endpoints was utilized. All that, subsequently approved by the FDA, who’s reputation is now crumbling at the foundation as a consequence of that decision, and many recent ones like it
As you now see, it’s not an effective public health strategy to prescribe an intervention that only transiently reduces mild symptoms, yet comes with a high adverse event profile compared to other treatments. The scientific thing to do would be prescribe a somewhat similar and efficacious intervention. Largely because the risk of myocarditis, thrombosis, VIT and arrhythmia should never be a trade off to avert mostly common-cold like symptoms. Make no mistake, Omicron BA1 & BA2 are mild for most. Of course, this segues into the next area of concern. That being, specific effective COVID-19 interventions/treatments.
There are therapeutics available like Paxlovid, Fluvoxamine, and Molnupiravir. These are outpatient treatments (pills) that can be taken at home if one believes they’ve been exposed, or are showing COVID symptoms. Moreover, Paxlovid and Molnupiravir can be obtained at many local pharmacies without a doctors prescription. That said, the total effectiveness against death and severe symptoms of both drugs combined is around 86%, whereas COVID vaccines lose almost all potency within months while running the risk of severe side effects.
At this point it is clear the right thing to do is shift attention from pushing ineffective mRNA vaccines, into providing early outpatient treatments as they are more effective and yield less severe side effects. After all, wouldn’t you rather an effective COVID treatment?
LETS CONNECT: