

Vaccination Can't Be The Main Answer Anymore- These 3 Things Need To Happen Immediately
Vaccination Can't Be The Main Answer Anymore- These 3 Things Need To Happen Immediately

Since mid-December of 2020, vaccines have been the main treatment used for protection against severe disease and death from COVID-19. However, now being 2 years into the pandemic, vaccines need to take a backseat while these 3 important areas are intensely focused on.
To begin, let’s set the table. As of today, only 65.6% of Americans have received their mRNA primary series (1st and 2nd dose), while only 45% of have received their 1st booster. Of course, the 2nd booster has recently been approved but will likely reach less arms than the aforementioned. That coupled with anxiety from new Israeli data most people are now are aware of revealing 31.4% vaccine effectiveness against symptomatic disease, implies America has lost confidence in COVID vaccines and is/has been ready to focus on other areas.

First area of focus. More older drugs need to be repurposed to treat COVID-19. Just so it’s clear, currently, there are some EUA approved COVID treatments available like Paxlovid, Molnupiravir, and Fluvoxamine. However, they’ve been very difficult for people to acquire from the pharmacy, doctors office, or hospital because of regulations imposed by the current White House administration, underproduction (supply/demand), and high cost (minus Fluvoxamine).
Be that as it may, the shortage and resulting inability to receive early COVID-19 treatment is an indication that the current White House Administration has some work to do, and that more treatment options are needed. That means, more money should be shuttled into randomized controlled trials for older drugs. As a side note, it’s not efficacious to solely rely on retrospective observational studies/meta-analysis like many have to justify using certain pharmaceuticals to treat COVID- there needs to be some appropriate RCT data. Considering the previously stated, solid RCT data may bridge the gap for Ivermectin, and hydroxychloroquine that have been proven to work in retrospective observational studies (but not in randomized controlled trials specifically for COVID), and anecdotally. These randomized controlled trials need to happen immediately so more options can be potentially available to the public. Sadly, political pushback is preventing appropriate funding of these studies from occurring.
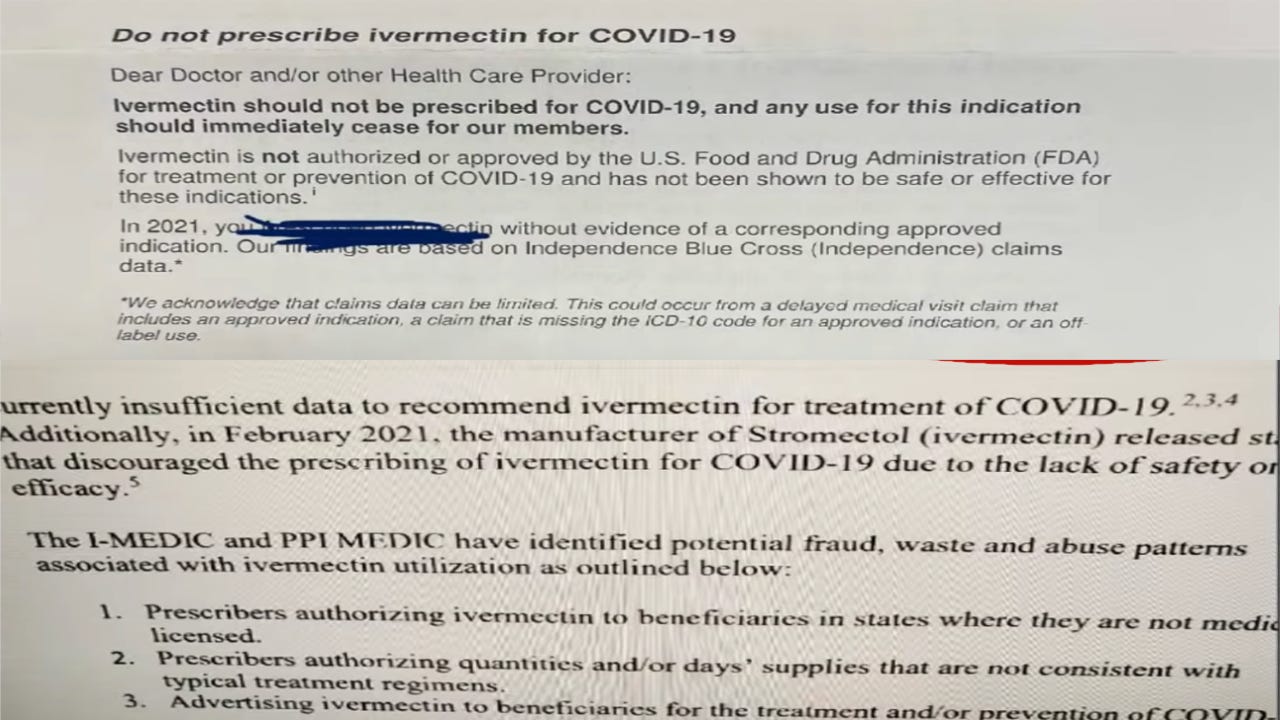
Second area of focus. Local health boards need to stop threatening to revoke physician’s licenses for using off-label drugs to treat COVID-19. Just so you understand, off-label prescribing is a frequent action utilized by many doctors, nurse practitioners, and physician’s assistants. Succinctly put, it means drugs used to treat specific diseases are prescribed for other illnesses when there’s some data to show they’re efficacious for both. Make no mistake, this doesn’t mean the drug can be officially prescribed for a disease, only sometimes on a case-to-case basis.
Largely, off-label prescribing is an autonomous action executed by clinicians at the bedside, and doesn’t involve the input of a 10-times removed public health authority. After all, what’s the point of a doctors nuance if a faceless agency dictates patient centered care?
Finally, speaking of older drugs, it’s clear issues surrounding Ivermectin & hydroxychloroquine remain politically charged which presents harrowing implications for the future of off-label prescribing. Considering the evidence, physicians need to be left alone to do what they do best. Medicine.
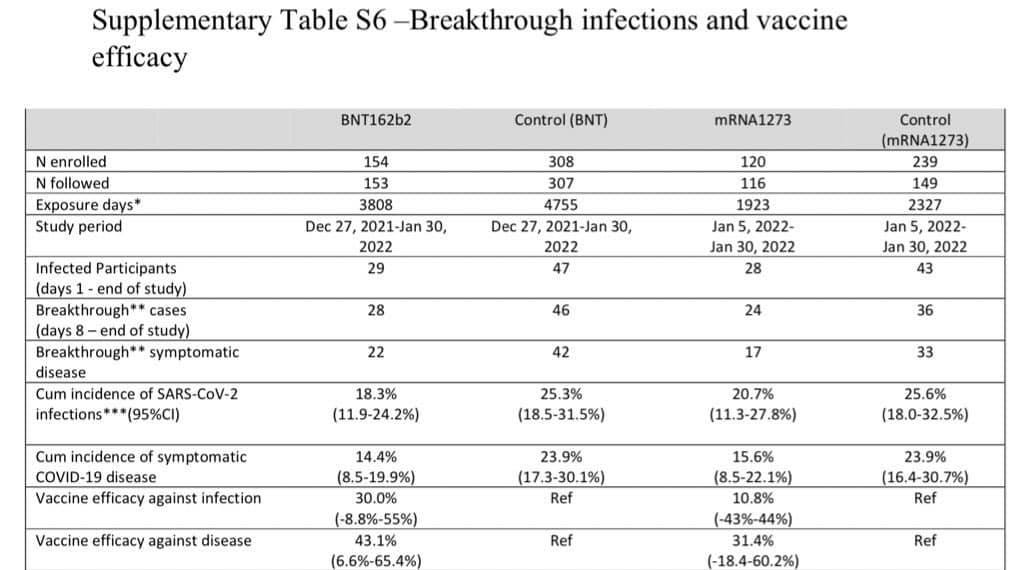
Third area of focus. Vaccines engineered against the original Wuhan strain are no longer effective for new variants, and Pfizer + Moderna refuse to updated their mRNA code, so administration needs to cease immediately. To give an example, a new Israeli study on a 4th dose revealed vaccine efficacy of 31.4% against symptomatic disease after only a few months of receiving the jab. Just to add some context, the bar for approval in the original Pfizer & Moderna clinical trials was around 50% efficacy.
Now, arguably the most important takeaway. At this point there are more variants a person has been exposed to than number of times they are allowed to vaccinate. That means most have been asymptomatically, or symptomatically infected with every COVID variant which has conferred more immunity than vaccination overall. As a result, robust protection against severe disease and death has been granted mainly from the virus, so it’s time that ineffective vaccines are moved away from the spotlight.
As you can see, between low public confidence in vaccines + plummeting efficacy, coupled with sparse drugs to treat COVID-19, it’s time Pfizer and Moderna take a back seat while other important areas are focused on.
LETS CONNECT:
Calling for more money to research old drugs? Really? The 70 trials of ivermectin are not enough? These positive results are just an accident? I have never seen more proof for a drug for a treatment, with such a big effect size. I don't think there is any. Considering this is all independent research, no big pharma to sponsor it.